
Why COVID-19 Is Here to Stay, and Why You Shouldn’t Worry About It
As many countries are going through another wave of infections, including some where the vast majority of the population has been vaccinated, many are starting to despair that we’ll never see the end of the pandemic. In this post, I will argue that, on the contrary, not only is the pandemic already on its way out, but the virus will be relatively harmless after it has become endemic. This is going to happen not because the SARS-CoV-2 will become intrinsically less dangerous, although it might, but rather because what made the virus so dangerous was that nobody had immunity against it, so once it has become endemic it will infect fewer people and even those who end up infected will be much less at risk. Moreover, I will explain that, despite widespread anxiety about the emergence of new variants and the danger of immune evasion, the fact that SARS-CoV-2 is mutating will not prevent this outcome because of the way immunity works. Finally, I will argue that, although some people are calling to pursue the eradication of SARS-CoV-2 (as we have done with smallpox), we almost certainly couldn’t eradicate it even if we wanted to and that even if we could it wouldn’t be worth it.
SARS-CoV-2 is going to become mostly harmless
You may have heard that, as they evolve, viruses necessarily become less lethal because it makes no evolutionary sense for them to kill the hosts on which they depend for their survival and reproduction, but this is a myth and it’s not what I’m saying. The claim I’m making is based on a much sounder and more straightforward argument. But to understand why it’s true, you first have to understand that, as the virologist Dylan H. Morris explained in a great essay, what made SARS-CoV-2 so dangerous is not so much its intrinsic characteristics but the fact that it was novel, which means that nobody in the population had immunity against it.1 Indeed, while the debate about whether SARS-CoV-2 was “worse than the flu” or “just like the flu” dominated the early phase of the pandemic and to some extent is still ongoing, this question is not even well-posed because there is no such thing as the dangerousness of a virus simpliciter. The dangerousness of a virus is always relative to a particular context. This should be obvious if you consider the impact that the availability of effective treatments can have on how much damage a virus does. For instance, HIV was initially devastating because it invariably killed the people it had infected within a few years after symptoms onset, but thanks to the development of effective treatments infected people can now live a relatively normal life, at least in the developed world where people can afford such treatments. HIV has not become any less intrinsically dangerous, but it’s undoubtedly far less dangerous in societies where effective treatments are easily available.
In the case of SARS-CoV-2 though, the key contextual factor is what proportion of the population has immunity against it. Immediately after the emergence of the virus, the population was immunologically naive, which means that nobody had immunity against it beyond that conferred by the innate immune system against any pathogen.2 The amount of damage and disruption caused by a virus can differ wildly depending on whether the population in which it’s introduced is immunologically naive to it. This is because, when nobody in the population has immunity, 1) the virus spreads more easily and infects more people because everyone is susceptible to infection and 2) when people get infected they have a much higher chance of developing a severe form of the disease because their immune system does not yet have any weapons specifically tailored to fight this virus. So the same virus, with exactly the same intrinsic properties, can do vastly more damage in a population that is immunologically naive than in a population where everyone has immunity against it, either because they have previously been infected or because they have been vaccinated. That’s one of the reasons why entire indigenous communities in America were almost completely wiped out by pathogens brought by Europeans, even though people in Europe had been living with the same pathogens for centuries or even millennia and, while they were not by any means harmless to them, they didn’t threaten their existence.3
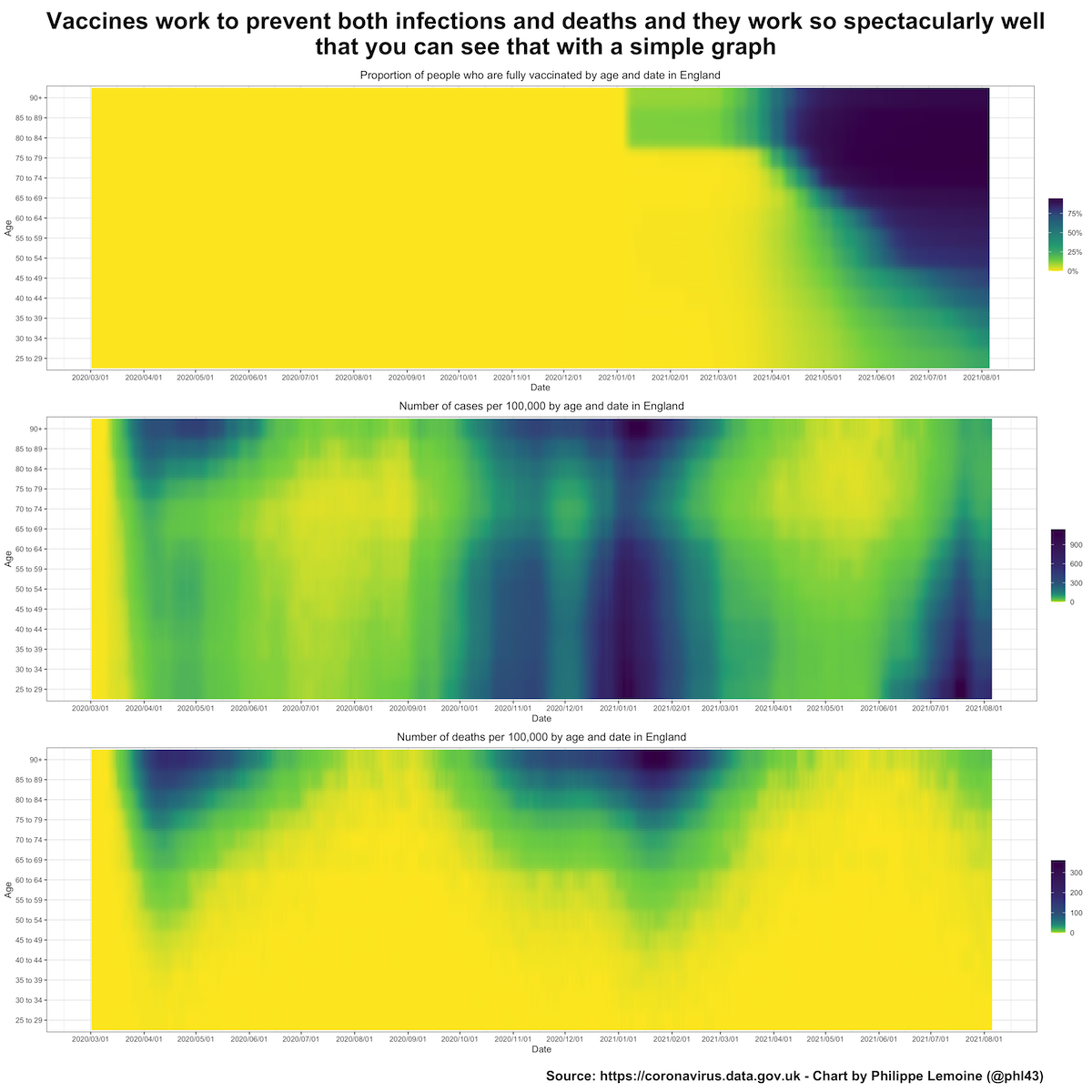
As more people get infected by SARS-CoV-2 or vaccinated against it, the virus will become endemic and continue to circulate following a seasonal pattern (because immunity whether acquired naturally or through vaccination is not 100% effective against infection and wanes over time), but the number of people who end up at the hospital or dead because of it will gradually decrease until we reach a sort of equilibrium.4 In some places, especially in developed countries where the vast majority of the population has already been vaccinated, this process is already well under way and you can see it on a simple chart:This is probably also true in other regions of the world, where infections usually played a bigger role than vaccination, and eventually it will be true everywhere, including in places such as Australia and New Zealand that have mostly been able to keep the virus out so far but won’t be able to do it forever as the virus becomes endemic in the rest of the world. Obviously, it’s preferable to build up immunity through vaccination rather than infections, but eventually everyone will get to the same point. The virus will become endemic and virtually everyone will have some immunity against it, at which point it will be relatively harmless and no longer cause the kind of damage we have seen during the pandemic. The whole process will take a few years, but again it’s already well under way in some places and this is where everyone is headed, dreams of eradication notwithstanding.
{kind=link}
In order to understand how this transition takes place and why the virus will be mostly harmless once it has become endemic and the population is no longer immunologically naive to it, I think it’s useful to work through a simple numerical example, which doesn’t purport to be a quantitatively accurate description of what is going to happen but can illustrate the process qualitatively and help people to grasp the underlying logic. Let’s consider a population of 10 million with 3 million people between 0 and 18 years old, 4 million people between 19 and 59 people and 3 million people 60 and over. Suppose that in that population a virus kills 0.05% of the people between 0 and 18 years old it infects, 0.2% of the people between 19 and 59 and 1% of the people 60 and over. Let’s also assume that, during the first year after it’s introduced in the population (which is initially immunologically naive to it), 25% of the population is infected and this doesn’t vary by age. In that case, we expect that during that year it will kill 25% * 3,000,000 * 0.05% = 375 people between 0 and 18 years old, 25% * 4,000,000 * 0.2% = 2,000 people between 19 and 59 years old and 25% * 3,000,000 * 1% = 7,500 people 60 and over died, for a total death toll of 9,875. That is a pretty sizable mortality, comparable to what many countries have seen during the first year of the COVID-19 pandemic, which given the assumptions I made should not come as a surprise to anyone.
Now let’s consider the same virus but in another population of 10 million or in the same population at a subsequent date where, because of vaccination and infections, the prevalence of immunity is only 25% among people between 0 and 18 years old, but 100% in the rest of the population.5 Let’s further assume that immunity is 80% effective against death and that effectiveness doesn’t vary with age, but that it’s not as effective against infection. Still, it offers some protection against infection, so the virus doesn’t spread as much as in a population where there is no immunity whatsoever. Let’s be more specific and assume that, over the course of a year, 15% of people between 0 and 18 years old, 10% of people between 19 and 59 years old and 5% of people 60 and over get infected.6 Finally, let’s assume that 75% of the children who get infected had no prior immunity, while 100% of the adults who get infected had some immunity since we have assumed that except for children everyone had immunity. In that case, we expect that 15% * 3,000,000 * (75% * 0.05% + 25% * (1 – 80%) * 0.05%) = 180 people between 0 and 18 years old, 10% * 4,000,000 * (1 – 80%) * 0.2% = 160 people between 19 and 59 years old and 5% * 3,000,000 * (1 – 80%) * 1% = 300 people 60 and over died, for a total death toll of 640. That’s only ~6.5% of the death toll in the immunologically naive population, yet by assumption the virus is exactly the same as before, but the population is no longer immunologically naive and this changes everything. For various reasons I won’t get into here, reality is far more complicated than this simplistic model, but it’s good enough to grasp the basic logic that governs the transition toward endemicity and get a pretty accurate idea of what is going to happen.7
Sooner or later, as a result of both infections and vaccination, virtually everyone will develop some immunity against SARS-CoV-2. This immunity will not always prevent infection, but even if someone who has been vaccinated or previously infected gets reinfected, they will typically develop only a mild form of the disease, because while still not perfect the protection against severe illness that immunity confers is better and doesn’t wane as quickly as protection against infection. Even the protection against severe illness will likely wane after a while, but this won’t really be a problem because, since immunity is much less effective against infection and new people are going to get born who are completely susceptible because they have never been infected yet and won’t be vaccinated, the virus will continue to circulate so most people will be reinfected every few years. Most people see that as a bug, but in a way, it may actually be a feature. Indeed, those reinfections will typically be mild because immunity protects well against severe illness, but they will update immunity and therefore ensure that, the next time someone is infected, this reinfection is also mild. As long as the virus is not eradicated, which as we have seen is not going to happen, we don’t want it to circulate too much, but we also don’t want it to circulate too little. Otherwise, too much time may elapse between two infections in the same person, in which case even the protection against severe illness conferred by immunity may have waned by the time they get reinfected.
Eventually most people will have a primary infection when they’re children, which is perfectly harmless and, together with subsequent infections, will protect them against severe illness later, when infection would be more dangerous if they didn’t have any immunity. Since once people have immunity, infections are generally mild, most people likely won’t even bother getting vaccinated because the probability of becoming seriously ill due to SARS-CoV-2 will be very small since 1) the risk of getting infected in the first place will be low because immunity still offers some protection against infection and the virus will circulate much less after it has become endemic and 2) even if they are infected they will typically be well protected against severe illness. Elderly people will be the exception because their immune system is compromised, so for them it will make sense to get a vaccine booster on a regular basis and I expect that it’s what most of them will do, as they already do against the flu. Once it has become endemic, which again will take a few years or even decades for the transition to be fully over, SARS-CoV-2 will become just another respiratory virus and will never cause the damages it has just wrought on us again. At last, it will have become “just like the flu”, except that it probably won’t be as bad as the flu if only because immunity will be more effective and longer-lasting.8 This may have already happened in the past with a coronavirus after the 1889-1891 “Russian flu” pandemic, which some now believe to have actually been caused by the emergence of HCoV-OC43, another human coronavirus that is now endemic and causes the common cold. It’s likely that SARS-CoV-2 will follow a similar path and end up being similarly harmless.
How I learned not to worry about variants and why you shouldn’t either
I have argued that, although SARS-CoV-2 is not going anywhere and that it wouldn’t be eradicated, things are looking up and that as the virus becomes endemic it would become mostly harmless. However, I know that presented with the optimistic picture I painted of what lays ahead of us, many people will react in disbelief because they think that emerging variants of the virus will get in the way of this quasi-idyllic scenario. Instead of seeing the wave of infections associated with the Delta variant as the last jolts of a pandemic on the way out as the transition toward endemicity takes place, they see it as a sign that, because new variants will keep emerging, we are going to be trapped in a never-ending cycle of waves of infections, each of them leaving scores of dead behind. Given that since the end of 2020 and the emergence of the Alpha variant in England, a wave of variantophobia has taken over the world, I can’t blame you if you worry that something like that might be true, but if that’s the case then I think you will feel much better after reading this section because the case against this variantophobia is very strong and we have every reason to believe that variants won’t prevent the scenario I described above from unfolding. First, before I say anything else, just taking another look at the chart about what just happened in England above should already assuage your worries somewhat, but there is more so please just bear with me for a little longer and I promise that you won’t regret it.
Variants are neither a new phenomenon nor something peculiar to SARS-CoV-2. Viruses constantly mutate and, as a result, variants of SARS-CoV-2 started to emerge long before the public became aware of that phenomenon a few months ago. While I do not doubt that mutations can result in different properties, as I have already explained previously, the picture is more complicated than what epidemiologists claim, especially when it comes to their claims about the advantage of transmissibility that, according to them, some variants enjoy. But the real concern people have about variants in the long-run is that they might evade pre-existing immunity, in which case we’d pretty much be back to square one. Indeed, the optimistic prediction I made about what is going to happen as the virus becomes endemic depends on the fact that, once everyone has acquired immunity against the virus, it will no longer kill a large number of people because immunity will ensure that it circulates less so fewer people will be infected and that even when someone is infected the infection will usually be mild. Obviously, if new variants emerge that can evade this immunity, this is not going to work and the pandemic will not end. But this is not going to happen and people who say otherwise are just talking nonsense.
In order to understand why, you must know a few things about how immunity works. Most people think of immunity as a black-or-white kind of thing: you either have it and you’re completely protected against both infection and severe illness or you don’t have it and you’re not protected against either. However, that is not how it works, the reality is more complicated. Immunity has several layers and comes in degrees. I have already noted that immunity against SARS-CoV-2 offered better protection against severe illness than against infection, but it’s even more complicated than that. For one thing, even if you have never been infected by SARS-CoV-2 and have not been vaccinated, it’s not true that you have no immunity against it. You have some immunity against it because your innate immune system is capable of fighting off even pathogens that you have never encountered. If this were not true, everyone who is exposed to SARS-CoV-2 would have died, but almost everyone survives and the overwhelming majority of people only have mild symptoms or no symptoms at all. It’s just that sometimes this innate immunity is not enough to clear the infection on its own before things get ugly, so it needs the adaptive immune system, which is responsible for mounting a more specific immune response to pathogens.
Unlike the innate immune system, which offers generic protection against pathogens, the adaptive immune system offers tailor-made protection against specific pathogens that it previously encountered. It relies mainly on two types of cells, B-cells and T-cells, that each play a different role, but in both cases they work by recognizing parts of proteins called epitopes expressed by the pathogen, which in the case of SARS-CoV-2 is a virus. B-cells have receptors that directly bind epitopes on the surface of the virus, then proliferate and create antibodies that can also bind those epitopes, which prevents the virus from infecting cells and helps other types of cells in the immune system to remove them. In the case of T-cells, on the other hand, recognition is a bit more indirect. Viral proteins are first broken up into short chains of amino acids called peptides inside cells that are called antigen-presenting cells (APCs).9 Those peptides are then bound to molecules known as the major histocompatibility complex (MHC) and the resulting MHC-peptides complexes are transported to the surface of the APCs where they are presented for recognition by T-cells.10 T-cells have receptors that bind different types of MHC-peptide complexes and, if they recognize one of them, they get activated and start going to work against the virus. This contributes to the immune response in various ways, but in particular sets in motion the process that will result in the destruction of the cells that have been infected by the virus.11 Here is a chart adapted from this paper that summarizes B-cell and T-cell epitope recognition:A key fact about both T-cells and B-cells is that, when they are activated, they don’t just set in motion a process that will help clear the infection currently ongoing, but also a process that will allow them to do that more quickly the next time they encounter the virus.
{kind=link}
You’re probably wondering why I’m telling you about all that, but don’t worry, you’re about to find out. In the case of SARS-CoV-2, antibodies seem to be crucial to protect against infection, which makes sense because if there are still many antibodies that can neutralize the virus around when someone is exposed to the virus again, it won’t even have the opportunity to infect cells and replicate. However, several studies have found that the number of antibodies against SARS-CoV-2 wanes relatively quickly after vaccination or a natural infection, so often immunity can’t prevent infection. But as we have just seen, the immune response is not limited to antibodies, let alone to the antibodies against SARS-CoV-2 that are still around by the time someone is exposed to the virus again. Upon a second exposure with the virus, T-cells whose receptors bind peptides from SARS-CoV-2 will go to work again, but this time they’ll be able to do it more quickly. This will ensure that, even if infection couldn’t be prevented, it will be cleared before things take a turn for the worst. Thus, T-cells play a key role in preventing severe illness and, unlike antibodies, neither B-cells nor T-cells specific to SARS-CoV-2 seem to wane quickly. In fact, according to various studies (including one which found that T-cells specific to SARS-CoV-1 were still present in the blood of people who had been infected 17 years ago), they likely stick around for years. So even though protection against infection seems relatively short, immunity likely confers protection against severe illness for a long time. But won’t new variants find a way to evade this pre-existing immunity and make even the protection against severe illness it confers ineffective? No, they almost certainly won’t, and T-cells are the reason why.
Indeed, T-cells mount a particularly robust immune response because they target a much greater number of epitopes than antibodies, so even the virus mutates to prevent antibodies resulting from a previous infection to bind it, this is unlikely to work against T-cells because the entire viral proteome of the virus, i. e. the complete set of proteins expressed by the virus, would have to be different. But SARS-CoV-2 mutates pretty slowly, so although new variants regularly emerge and will continue to do so in the future, most peptides from the virus will remain the same and therefore T-cells will still be able to recognize them. Indeed, the peptides that are bound to MHC molecules and presented on the surface of antigen-presenting cells are very short chains of between 8 and 25 amino acids (depending on the class of MHC to which they are bound), so they are unlikely to change even as the virus mutates. Since it mutates slowly, it’s kind of as if the virus were trying to win the lottery by just buying a handful of tickets, each of them with a very low probability of winning the jackpot. If it bought 500 of them, the probability that one of them is a winning ticket may be reasonably high, but since it only buys 8 to 25 of them in each case it’s very low. Moreover, even if one amino acid changes, this is usually not enough to prevent T-cell receptors from binding, so in this case having a winning ticket does not even guarantee that the virus will actually pocket any money. Of course, it will sometimes happen, but T-cells target hundreds of epitopes from SARS-CoV-2, so it won’t really make a difference to the overall immune response they mount against the virus. T-cells just take the recommendation that you shouldn’t put all your eggs in the same basket very seriously.
This looks fine in theory, but reality has a way of frustrating our theoretical expectations, so does it also work in practice? Yes, it does, it works exactly as theory predicts. A recent study examined the impact of SARS-CoV-2 variants on T-cell reactivity and found that, depending on the type of receptor, between 93% and 97% of the hundreds of previously identified T-cell epitopes were not affected by mutations in the variants of concern. Now, all epitopes do not contribute equally to the immune response mounted by T-cells, so in theory it could be that while only a handful of them were affected by mutations in variants of concern, they happened to be epitopes that were disproportionately involved in the T-cell response. But the authors checked and found that fully conserved epitopes accounted for on average 91.5% of the response, so this isn’t the case. Again, keep in mind that even for the handful of epitopes that were affected by mutations, it doesn’t mean that receptors from a previous infection are no longer capable of recognizing them. In any case, the study also found there was no statistically difference in reactivity of T-cells from people who had acquired immunity against the virus, whether it was through vaccination or a natural infection. It doesn’t mean that, had the sample been larger, a statistically significant difference wouldn’t have been found, but it means that at worse the loss of reactivity was small and possibly non-existent, which again is exactly what we’d expect based on the theoretical considerations. It may be that, although T-cells target hundreds of epitopes and SARS-CoV-2 is mutating slowly, after a long enough period of time it will have mutated enough that T-cells won’t be able to mount a strong enough immune response to protect against severe illness. But remember that SARS-CoV-2 is going to continue to circulate and that people will likely get reinfected every few years, so their immunity will be updated when they are, ensuring that any subsequent infections will also be mild.
But there is another reason almost nobody is talking about why it’s unlikely that we’ll see substantial immune evasion with T-cells. As I explained above, T-cells don’t recognize epitopes directly on the surface of the virus, but rather bind complexes formed by MHC molecules and peptides on the surface of antigen-presenting cells. Now, different MHC molecules can bind different peptides, which are then presented for recognition to T-cell receptors. As it happens, the region of the human genome that is responsible for the production of MHC molecules is the most polymorphic in the entire human genome, which means that even in the same population different individuals usually have different MHC molecules that can bind different epitopes from the virus before presenting them to T-cell receptors on the surface of antigen-presenting cells. This fact has been confirmed in the case of SARS-CoV-2 by another study that identified potential T-cell epitopes from the virus and used computational methods to predict their binding affinity with the MHC molecules produced by the different variants of the genes that code for them in human populations. The authors found there was significant variation in the epitopes derived from SARS-CoV-2 involved in T-cell response both across individual within the same population and between populations, although this variation wasn’t predicted to affect the overall level of response across individuals or populations.12 This is very important because it means that, even if the virus acquired mutations that allowed it to evade T-cell immunity in one individual or population, it typically wouldn’t help it evade T-cell immunity in another individual or population, which makes T-cell immune evasion even more unlikely.
The bottom line is that, if you’re the virus, T-cells are your worst nightmare. Getting ahead of antibodies is pretty easy and some variants of concern already do it to some extent, but T-cells are a completely different story and will be a much tougher nut to crack for the virus. As we have seen, we have very good theoretical and empirical reasons to expect that, in the war between the virus and T-cell immunity, not only is the latter going to win but it won’t even break a sweat doing it. It’s important to understand that, in that respect, SARS-CoV-2 is no different than other viruses and other viruses also have a hard time dealing with T-cell immunity. Indeed, as the authors of the study that examined the impact of SARS-CoV-2 variants on T-cell reactivity note, immune evasion at the level of T-cell response has never been reported for acute respiratory infections. People worry about variants because they hear that antibody response is not as effective against them, so they imagine that eventually another variant will emerge against which immunity will be completely ineffective, but that’s because they don’t know that antibodies are just one part of the immune response against SARS-CoV-2. Immunity has another layer depending on T-cells and, not only has this layer remained unaffected by mutations of the virus so far, but as we have just seen we have very good reasons to think it will continue to be true in the future.
As I noted above, it’s likely that SARS-CoV-2 will follow a trajectory similar to that of the other human coronaviruses (which are already endemic), so it’s particularly interesting to know that what I’m predicting for SARS-CoV-2 is exactly what is already happening with those human coronaviruses. A recent study examined the recent evolution of HCoV-229E, one of the four human coronaviruses that are already endemic, and found that its spike, the protein that allows the virus to enter cells and infect them, had undergone several mutations between 1984 and 2020. They used sera collected on recovering patients at various points during that period to test how well the antibodies they contain were able to bind reconstructed spikes of the virus from 1984, 1992, 2001, 2008 and 2016. What they found is that antibodies in sera collected at one date were able to find effectively the spikes that were found on HCoV-229E before that date, but not or not very effectively the spikes that were found on the virus after that date, which shows that HCoV-229E had mutated to evade antibody binding, which is already what we’re seeing in SARS-CoV-2. But HCoV-229E remained mostly harmless during that period, which is presumably because while people’s antibody response against it became less efficient due to mutations in the spike, T-cell immunity remained largely unaffected. This is exactly what we’re seeing with SARS-CoV-2 so far and we have every reason to believe that it will continue to be true in the future. The only difference is that, in the case of HCoV-229E, nobody bothers naming the variants and people aren’t freaking out because they think immunity will stop working against them. Again, SARS-CoV-2 is just another respiratory virus, what made it so devastating is that it was novel.
SARS-CoV-2 is not going anywhere
Some people insist that we can’t “live with the virus” and that we must therefore pursue a policy of eradication. They often draw a parallel with smallpox and say that we should do the same thing with SARS-CoV-2 that we did with that virus, which after plaguing mankind for thousands of years was finally eradicated in 1980. This parallel is extremely misleading though, because smallpox differs from SARS-CoV-2 in very important ways, which made eradication possible though difficult in the case of the former but make it very unlikely in the case of the latter. Before I get into that, it’s worth noting that to date only two infectious diseases have ever been successfully eradicated (smallpox in humans and rinderpest in cattle), which speaks to how difficult this sort of enterprise is. This is not for lack of trying, as several other infectious diseases have been targeted for eradication, but those efforts have not succeeded yet. Polio seems on the verge of eradication and probably will be eradicated soon, but isn’t yet. Even in the case of smallpox, eradication took decades. You might take this to suggest that, while SARS-CoV-2 will not be eradicated overnight, we might pull it off eventually if we really commit to it. But I don’t think it’s going to happen because again SARS-CoV-2 is very different from the viruses that cause smallpox or polio.
First, while I think there is no doubt that vaccines against SARS-CoV-2 protect against infections and not just severe disease (as we have seen above), I think it’s equally clear that the protection it offers against infection is far from perfect and that people can get infected even if they have been vaccinated. There is also growing evidence that, while it does not disappear almost immediately as some people had initially suggested based on weak evidence, the protection against infection conferred by vaccination is waning relatively quickly. As this study showed, the same thing is true for the immunity against endemic human coronaviruses induced by natural infection, so this is not particularly surprising. According to the COVID-19 Infection Survey, based on a random sample of the population in the United Kingdom, more than 90% of people had antibodies against SARS-CoV-2 in June, but it didn’t prevent a gigantic third or fourth wave (depending on how you’re counting) from ripping through the country in July. The same thing just happened in Iceland, where more than 90% of the population over 16 has received at least one dose of vaccine. As we have seen, this is not really a problem because thanks to vaccination and naturally acquired immunity mortality remained low, but it suggests that even mass vaccination within a short period of time cannot stop the virus from circulating. The vaccine against smallpox, on the other hand, probably confers lifelong protection against infection and the same thing seems to be true about naturally acquired immunity. Basically, in order to get rid of smallpox, we “just” needed to vaccinate everyone in their childhood and that was it. The same thing is true with polio.
So this means that, in order to eradicate SARS-CoV-2, we’d have to vaccinate the entire population every year for several years in a row and even that would probably not be enough.13 That’s a much larger effort than what we had to do to get rid of smallpox, yet even that comparatively simple endeavor took decades. Who can seriously believe that we’ll be able to sustain that effort for the years or even decades that it would take to eradicate the virus, when we aren’t even able to do it in the middle of a pandemic that just killed millions of people? This is a pipe dream, it will never happen. Indeed, convincing or coercing people to get vaccinated is going to become even harder, because as I have explained the virus will be mostly harmless once it has become endemic. If you think it’s hard to convince people to get vaccinated or politically difficult to coerce them to do so while people are dropping dead by the thousands, which it most certainly is, wait until the mortality caused by SARS-CoV-2 is divided by a factor of 20 or something. It’s pointless and wasteful to pursue a policy that has no realistic chance of succeeding, but that’s exactly what people who are calling to eradicate SARS-CoV-2 are doing. Not that it will make any difference, to be clear, because the same reasons that make this project a fantasy will ensure that calls to carry it out will remain unanswered.
Again the comparison with smallpox or even polio is extremely misleading here. Smallpox is one of the most lethal pathogens in history and has probably killed hundreds of millions of people in the last 100 years of its existence alone. It’s painfully obvious that the incentives are completely different in the case of SARS-CoV-2. Even with polio, whose infection fatality rate is similar to SARS-CoV-2, the incentives are very different because it mostly kills or maims children. Does anyone really expect that people are going to be as motivated to eradicate a virus that mostly kills elderly people as they are to get rid of a virus that kills or paralyzes children? Moreover, as I already noted, in the case of polio, you just have to administer a few shots to people when they’re very young children and you’re done with it. The comparison of SARS-CoV-2 with other pathogens can be illuminating in some cases, but comparing it to smallpox or even polio to suggest that we could eradicate it and that it’s a realistic possibility is extremely misleading. Even if we granted for the sake of the argument that it could be done if we committed enough resources to the effort, it’s totally unrealistic to expect that we ever will, because the incentives aren’t right.14
There are other differences between SARS-CoV-2 and smallpox or even polio that make it far more difficult to eradicate the former. In particular, smallpox and polio only infect humans, but SARS-CoV-2 can also infect animals and frequently does. While the evidence of animal-to-human transmission is so far very limited, I think it’s mostly because the studies that have found evidence that animals could be infected by SARS-CoV-2 were not designed to answer that question. If the virus becomes endemic in some animal populations that are frequently in contact with humans, then even if we somehow managed to temporarily eradicate it from human populations, animals would just reintroduce it and we’d be back to square one. At least one animal reservoir has already been found in the white-tailed deer population in the US, so this isn’t a purely theoretical worry. What this means is that, in order to permanently eradicate SARS-CoV-2 from human populations, we’d probably have to vaccinate wild animals. This can be done and has been done in some countries such as France, where a program to vaccinate some wild animals against rabies was undertaken, but it just makes eradication even more difficult and costly, which in turn makes it even more unlikely that we’ll even try, let alone succeed.
Conclusion
The pandemic is on its way out, but SARS-CoV-2 is here to stay. Fortunately, as everyone develops immunity to it (whether through vaccination or natural infection), it will soon no longer be a major problem anymore. The virus will continue to circulate, but much less than during the pandemic and, even when people are infected, the infection will typically be mild. In the future, almost everyone will get infected for the first time during their childhood, which is harmless and will protect them against severe illness when they are reinfected.15 The virus will continue to mutate and some of those mutations will favor immune evasion, but while this will allow it to infect people who have already been infected or vaccinated more easily, immunity should continue to protect against severe forms of the disease, thanks in particular to the role played by T-cells. This is likely what happened with other human coronaviruses, which are already endemic and typically cause a cold in the people they infect. To the extent that immune evasion occurs, it will be very gradual and the fact that most people will be infected every few years will update their immunity, ensuring that subsequent reinfections will also be mild. The most vulnerable people, whose immune system doesn’t work very well and could use some help to be ready in case of infection, can get a vaccine booster from time to time. The virus will still kill people, as the flu does, but it will never cause the same amount of disruption again. The hardest part of what lays ahead may be to convince people who have been traumatized by the pandemic that it’s over and that restrictions are no longer necessary.
P. S. I realize that, while it doesn’t exactly say that, this post makes it sound as though the only reason why protection against infection appears to have been waning is that new variants with mutations in the spike that allow them to prevent antibodies from binding have emerged, so to be clear that’s not what I’m saying. I was focusing on immune evasion, because that’s what people seem most worried about, but another reason why protection against infection is probably waning is that antibody levels progressively fall after infection. Moreover, as someone pointed out to me, so does the number of T-cells specialized against SARS-CoV-2 and I’m sure the same thing is true with B-cells, so as time goes by it also takes longer for the adaptive immune system to mount a response upon exposure to the virus. I also didn’t mean to suggest that mutations in the spike make antibodies completely inefficient. The point I wanted to make is just that, even if a variant is able to evade humoral immunity to a large extent, T-cell immunity should still work just fine against it and eventually the immune system should be able to mount a very effective response to infection, even if the fact that T-cell levels also wane means that it will take longer as the time since the last infection increases.
![]()
- 1
As some studies suggest, there was probably some cross-immunity due to prior exposure to seasonal human coronaviruses, so this claim is not exactly true, but clearly this immunity was very limited.
- 2
Biologists make a distinction between the innate immune system and the adaptive immune system. The former offers generic protection against pathogens that invade the body and can effectively deal with most of them, while the latter offers protection against specific pathogens that have been previously encountered. As I noted above, there was probably some adaptive immunity against SARS-CoV-2 in the population due to the similarity of parts of the proteins expressed by the virus with those of endemic human coronaviruses, but again it was very limited.
- 3
Another reason is that natural selection had probably favored alleles that protect against those pathogens in Europeans precisely because they had lived with them for so long, whereas this was not the case in America where indigenous populations had separated from other human populations before the emergence of those diseases, which probably occurred during and after the neolithic when animals were first domesticated.
- 4
The notion of endemic equilibrium has a precise mathematical definition in epidemiological models, but while those models may be useful to describe some aspects of this process in a stylized manner, I think they bear little connection to reality and use the term in a more informal sense.
- 5
This is the kind of situation you would expect in a population where the virus has become endemic, almost everyone is infected for the first time during their childhood, immunity wanes over time but people get reinfected or vaccinated every few years.
- 6
This is the kind of situation you would expect if old people got vaccinated regularly because they know they are vulnerable. You would expect the virus to circulate more among children since, by assumption, more of them are susceptible to infection.
- 7
If you want to see a more realistic attempt at modeling the transition to endemicity, which tries to predict how long it will take depending on factors such as how fast the protection against infection conferred by immunity wanes and the basic reproduction number of the virus, I encourage you to read Lavine et al. (2021). I wouldn’t take very seriously their quantitative estimates, because the model still ignores many complications and the specific results are sensitive to various semi-arbitrary assumptions they make, but there is every reason to think their qualitative conclusions, which are consistent with the prediction I make below about what is going to happen once SARS-CoV-2 has become endemic, are correct because they just rest on the basic logic I have just explained.
- 8
Indeed, influenza mutates faster than SARS-CoV-2 due to the absence of a similar proofreading mechanism during replication and because it has a segmented genome that makes recombination between various strains easier, which makes it harder for immunity to clear infection and explains why vaccines against the flu quickly become obsolete.
- 9
The terminology can be a bit confusing, so it may be useful to clarify it. Epitopes are the parts of viral proteins that are recognized by the adaptive immune system, whether they are still part of the protein when this recognition takes place or have been broken up and are no longer part of it. In the case of B-cells, they are recognized directly on the protein that is still intact on the surface of the virus, but in the case of T-cells this recognition takes place after the viral proteins have been broken up into peptides. So peptides can be epitopes when they are presented on the surface of APCs for recognition by T-cells, but epitopes need not be peptides and peptides need not be epitopes.
- 10
There are different classes of MHC molecules that are found on different kinds of APCs and are recognized by different types of T-cells, but this is not important for what I’m trying to explain.
- 11
B-cells are APCs and therefore present MHC-peptide complexes to T-cells, which in turn stimulate the proliferation of B-cells specific to the relevant peptides and the production of antibodies that can bind them directly on the surface of the virus, so T-cells and B-cells are not entirely distinct parts of the immune system but interact in complex ways to produce the immune response.
- 12
This result still held when they looked at potential T-cell peptides derived from individual proteins expressed by the virus rather than the entire viral proteome, so even if peptides derived from specific proteins are more important to the T-cell response than others, this response will still rely on different epitopes in different individuals and different populations. In particular, this is true for epitopes derived from the spike protein, which is the one used by the currently available vaccines to induce immunity.
- 13
Perhaps this will change as new, more effective vaccines are developed, but I wouldn’t hold my breath, especially since as I have argued SARS-CoV-2 is going to become far less dangerous, so pharmaceutical companies will have less incentives to invest money into research and development for better vaccines against it.
- 14
You may think that, although eradicating SARS-CoV-2 would be extremely costly and difficult, it would still be cost-effective given the expected death toll of COVID-19 in the long-run and you may even be right despite the fact that it’s going to become far less dangerous once it’s endemic. But this wouldn’t change the fact that it’s almost certainly not going to happen because, as we have seen during the pandemic, decision-makers are hardly utility maximizers. Thus, when I claim that eradication of SARS-CoV-2 is not desirable, I’m not committing myself to the view that, even if people were perfectly rational, such a policy wouldn’t pass a cost-benefit test (although I think it probably wouldn’t), but only to the weaker claim that it wouldn’t in the actual world because the lack of incentives to pursue this policy lowers the probability of success and increases the cost.
- 15
At the moment, many people want to vaccinate their kids, but I doubt it will still be the case in a few years when the panic induced by the pandemic has subsided and people have realized that SARS-CoV-2 is harmless to